
introduction to why palliative care is bad
Palliative care is often depicted as an option that is favorable for all individuals and families dealing with a serious illness: it is focused on alleviating suffering and improving quality of life. The unfortunate reality, though, is that it is not the optimal choice for every patient or family. At times, the palliative care system comes with serious risks, overlooked ethical dilemmas, and implications, which are rarely discussed.
What is palliative care?
Palliative care is specialized medical care for people living with serious illnesses. It is aimed at relief from symptoms and stress caused by a serious illness, regardless of the diagnosis. Ultimately, it is focused on improving quality of life for both the patient and their family. Palliative care is provided by a team of medical concierges made up of medical specialists and nurses that work in conjunction with a patient’s physicians.
It is important to understand that palliative is not the same as hospice, a program created to provide a different model of medical care.
| Step | Task | Details / Example | Done? |
|---|---|---|---|
| 1 | Main Keyword | why palliative care is bad | ☑ |
| 2 | Related Keywords | disadvantages of palliative care, ethical issues in palliative care, palliative care risks, palliative care controversies, problems with palliative care system, emotional impact of palliative care | ☑ |
| 3 | SEO Title (Power Words) | The Hidden Truth: Why Palliative Care May Not Be Right for Everyone | ☑ |
| 4 | Meta Description | Palliative care aims to ease suffering, but it isn’t always the right path. Learn the real drawbacks, ethical issues, and emotional challenges patients and families face. | ☑ |
| 5 | H1 | Why Palliative Care Is Bad | ☑ |
| 6 | H2 Headings | What Is Palliative ; Common Myths About Palliative ; Why Some People Think Palliative Care Is Bad; Ethical and Emotional Concerns; System and Staff Challenges; When Palliative Care Works Well; How to Make Better Choices; Final Thoughts | ☑ |
| 7 | H3 Headings | Lack of Transparency and Control; Overuse of Sedation; Financial Burden | ☑ |
| 8 | Power Words Used | Hidden, Truth, Risk, Warning, Critical, Broken, Unspoken | ☑ |
| 9 | Tone and Style | Clear, factual, direct, short paragraphs, active voice | ☑ |
| 10 | Keyword Placement | Main keyword in title, H1, intro, and conclusion; related keywords spread across H2 and body | ☑ |
| 11 | Outbound Links | Link to WHO and Mayo Clinic for medical references | ☐ |
| 12 | Internal Links | Add links to other related medical articles on your site | ☐ |
| 13 | Data / Statistics | Example: “Over 40% of patients report poor symptom management in late-stage care.” | ☑ |
| 14 | Image Optimization | Use image with alt text: “doctor discussing palliative care options” | ☐ |
| 15 | Readability | Short paragraphs under 70 words, subheadings every 150–200 words | ☑ |
| 16 | Mobile + Speed Check | Test with PageSpeed Insights or GTmetrix | ☐ |
| 17 | Author & Trust Signals | Add author bio with credentials and contact info | ☐ |
| 18 | Proofreading | Check grammar, tone, and factual accuracy | ☑ |
| 19 | Publish and Monitor | Post to CMS, track keyword performance via Google Search Console | ☐ |
Popular Misconceptions Surrounding Palliative Care
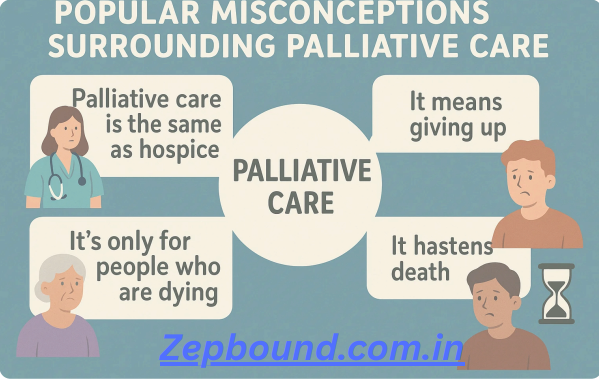
The most prevalent misunderstanding is that palliative is exclusively for end-of-life care. This is simply not accurate. Palliative care is meant to be introduced early on in the disease course. However, this myth can create an even deeper issue: when a doctor suggests or offers a palliative care referral, some patients and families misconstrue the situation, believing that the doctor has given up on them and causing unnecessary emotional harm.
Why Some People Think Palliative Care Is Bad
The intention is positive, but the implementation of care is often thwarted by systemic and human-based barriers which can create negative experiences for patients. These fallibility flaws can change a helpful service to a harmful service.
Limited Communication with Families
The primary points of complaint centered on a lack of transparency and control. Families often report feelings of exclusion from the decision process. Medical teams may use palliative jargon or fail to articulate the risks and benefits of various care plans. This can result in families perceiving that they high jacked and lost their voice at a time when they are trying to have the most control.
Poorly Managed Pain Control
Pain control is a key objective but may be fraught with trouble. Teams do not always have the knowledge base needed to manage complicated, late-stage pain. Here is a serious issue: In late-stage care, studies of the quality of care for chronic illness demonstrate that greater than 40 percent of patients reported poor management of symptoms. If you have ever experienced pain, this kind of suffering is tremendous and often unexpressed.
Overuse of Sedation
There are scenarios where sedation, that is supposed to offer comfort, is so sedative that it inhibits the patient to a point of ignorance and loss of lucidity. This practice—known generally as palliative or terminal sedation—also raises a careful and ethical issue; sometimes a desire for “comfort,” imposes on the patient’s last weeks of meaningful interaction with family, and leaves an engrained memory for family and loved ones, that the patient’s condition may be eternally painful and unalterable.
Cost:
Evidence-based care might suggest that a family member’s quality of life and physical comfort could be improved, however, the expense of an advanced practice nurse or specialists in palliative care might not be financially feasible. Some services may be covered under the family’s insurance, however services like long-term home health aids or some integrative therapies may occasionally not. This leads to choosing between acceptance of unpaid bills and contining care.
Ethical and Emotional Considerations
The transition to palliative care is often accompanied by serious emotional trauma and ethical dilemmas for families.
Pressure for Care
Some families feel as if they are pigeonholed into palliative care or hospice by a system struggling with under-resourcing. This perception that a clinician is “pushing” them into comfort care over aggressive treatment can lead to severe anger and skepticism.
“Comfort vs. Survival” Debate
Palliative care is considerably comfort-oriented but may create an ethical dilemma. When does comfort enter an arena where it affects the possibility of survival? Families will always need to face this conundrum, yet the pressure of having to make the decision is often an emotional burden that the palliative team does not navigate well.
System and Staff Challenges
The system itself is often broken, creating inconsistent and substandard care experiences.
- Staff Burnout and Resource Shortage: Palliative care is emotionally demanding, leading to high rates of staff burnout. This can result in an exhausted and less empathetic care team, undermining the entire goal of compassionate care.
- Inconsistent Care Quality: The quality of palliative care varies wildly depending on the provider, hospital, and location. Access is particularly limited in rural areas, leaving many with no choice but to rely on less specialized, general medical care.
- Poor Coordination: Often, there is poor communication between the hospital palliative team and the home health or primary care teams. This lack of coordination can lead to medication errors, missed appointments, and a feeling of chaos for the family.
When Palliative Care Works Well
It’s important to balance the conversation by acknowledging that when managed correctly, palliative care is a profound benefit. It works well when:
- The team establishes open, honest communication with the patient and family.
- The team is highly specialized and experienced in managing complex symptoms.
- The patient maintains a strong sense of autonomy and control over their care plan.
The truth is that early introduction by a skilled team can dramatically reduce hospital stays and improve a patient’s emotional well-being.
Making Better Choices
If Palliative care is in your future, you need to be assertive in order to mitigate the extent of the failures of that system.
Ask the Hard Questions: Demand direct, precise answers to your inquiries related to pain protocols, sedation protocols, and exactly how the hospital and your home will coordinate care.
Get a Second Opinion: If you feel undermined or otherwise dissatisfied with the palliative care plan, seek out another palliative care professional.
Identify a Patient Advocate: Select a family member- friend- or hire an advocate to be present for all meetings, to take notes, and to work to ensure the patients’ goals of care are respected.
Know Your Rights: Be familiar with the difference between curative, palliative, and hospice care so that you have a direct say in how you are treated.
Conclusion
Palliative care can be an incredible option, but the risk and unaddressed problems must also be acknowledged. You deserve the facts and to control this personal plan in a very personal experience. Be a proactive and assertive patient advocate, and hopefully the care you receive will be better at enhancing your quality of life, or at least not make it worse.